GENERAL MEDICINE CASE DISCUSSION.
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box.








A 65 year old patient came to the casualty with the chief complaints of :
1. Fever 1 month back
2. Cough since 20 days
3. Shortness of breath since 20 days (class II - class III) according to NYHA classification, not associated with orthopnea/PND.
4. Fever since 20 days , not associated with chills and rigor.
Patient was apparently asymptomatic 20 days back, then he developed fever which was insidious in onset, gradually progressive and subsided on taking medication.
Complain of cough , associated with sputum , yellowish in colour, non blood tinged, non foul smelling.
Not a k/c/o DM, HTN, asthma, TB.
Patient is on Tab OLANZEPINE 5mg, Tab ESCITALOPRAM -10mg since 2 years due to personality disorder.
Vitals on admission :
Temperature - 97 F
Pulse rate - 83 BPM
Respiratory rate -16 cpm
Blood pressure - 140/90 mm Hg
SpO2 - 99% at room air.
On examination :
Patient is irritable i
CVS - S1 S2 heard, no murmurs
RS - NVBS present
CNS - NAD
P/A - soft, non tender
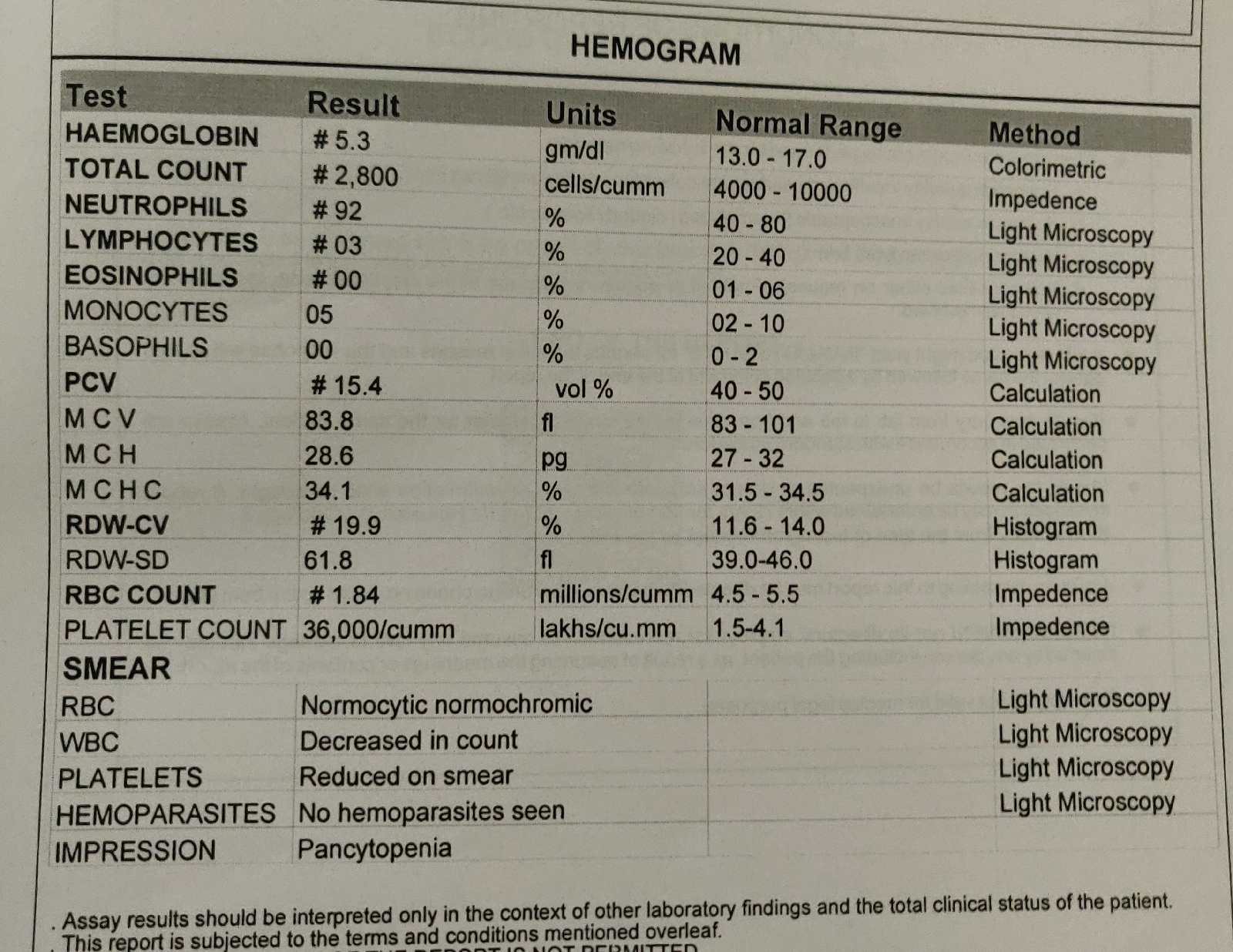
INVESTIGATIONS :






Serology was found to be negative.
USG Abdomen-
1. Right grade II RPD
2. Left grade I RPD
3. Mild Splenomegaly
Provisional diagnosis : COMMUNITY ACQUIRED PNEUMONIA OF RIGHT LOWER LOBE WITH PANYTOPENIA.
? AKI ON CKD.
Treatment :
1. O2 supplementation if SpO2<90%
2. Inj NEOMOL 100ml / IV/ if temperature> 101.1 F
3. Tab DOLO 650mg /PO/BD
4. Syp ASCORYL 10ml/PO/BD
5. Nebulization with IPRAVENT and BUDECORT - 6th hourly
6. Inj PAN 40mg /IV /OD.
On 24/11/2021,
S-cough with expectoration+,pt is standing up and micturating on the floor, sleep:pt woke up every hour and randomnly stood beside the bed .
no fever spike
O- conscious, intermittent coherent.
orientated only to person.
speech-slurred
memory -couldnt be elicited.
afebrile-
PR-121/min
BP-130/80mmhg
cvs:s1,s2+
r.s: bae+coarse crepts end insp,b/l ll, rt>lt
intermittent end exp wheeze +
spo2 on room air:94%
p/a:soft nt
BUN/creat:36.6(pre renal)
output: 1200ml till last night,not measured after that
usg-mild spleenomegaly.
A- B/L lowerlobe consolidation secondary to ? community acquired pneumonia
pancytopenia secondary to ?infection ? spleenomegaly.
AKI (pre-renal ) on ckd
h/o using antipsychotics since 2.5 years
P-inj ceftriaxone 1g/iv/bd
ivf -ns,rl@100ml/hr
neb with ipravent, budecort
syp ascoryl 10ml/po/tid
tab dolo 650mg/po/bd
with holding antipsychotics as per psychiatry consultation orders.
On 25/11/2021,
S - Patient is irritable
Fever spikes present
O - Patient is irritable, oriented only to person
Speed - slurred
Temperature - 99 F
PR - 83bpm
BP - 120/70mm Hg
RR - 22/min
CVS - S1 S2 +, no murmurs
RS - NVBS heard, crepts present in right IAA, ISA
SpO2 - 98% at room air
GRBS - 105 gm/dl
I/O - 700/950 ml
A : Community Acquired Pneumonia in right lower lobe with pancytopenia with AKI on CKD
P :
1. O2 supplementation if SpO2 < 90%
2. Tab AZITHROMYCIN 500mg PO/OD
3. Tab PAN 40mg PO /OD
4. Tab DOLO 500 mg PO / TID
5. Nebulization with IPRAVENT and BUDECORT every 6th hourly
6. Syp ASCORYL 10ml PO/ TID
7. Tab OLZIC 5mg / PO H/S
8. Vitals monitoring
On 26/11/2021 :
S - Patient is irritable
Fever spikes present
Thrombophlebitis present
O - Patient is irritable, oriented only to person
Speed - slurred
Temperature - 99.5 F (febrile)
PR - 98bpm
BP - 120/70mm Hg
RR - 22/min
CVS - S1 S2 +, no murmurs
RS - NVBS heard, bilateral crepts present in right IAA, ISA
SpO2 - 98% at room air
GRBS - 119 gm/dl
I/O - 700/950 ml
A : Community Acquired Pneumonia in right lower lobe with pancytopenia (resolving) with fever under evaluation with AKI on CKD
P :
1. O2 supplementation if SpO2 < 90%
2. Tab AZITHROMYCIN 500mg PO/OD
3. Tab PAN 40mg PO /OD
4. Tab DOLO 500 mg PO / TID
5. Nebulization with IPRAVENT and BUDECORT every 6th hourly
6. Syp ASCORYL 10ml PO/ TID
7. Tab OLZIC 5mg / PO H/S
8. Vitals monitoring
9. Fever Charting 4th hourly.
27/11/2021 :
Unit 1
S - Patient is irritable
Fever spikes present
Passed stools
O - Patient is irritable, oriented only to person
Speed - slurred
Temperature - 99.5 F (febrile)
PR - 89bpm
BP - 120/70mm Hg
RR - 22/min
CVS - S1 S2 +, no murmurs
RS - NVBS heard, bilateral crepts present in right IAA, ISA
SpO2 - 98% at room air
GRBS - 119 gm/dl
I/O - 700/950 ml
A : Community Acquired Pneumonia in right lower lobe with pancytopenia (resolving) with fever under evaluation with AKI on CKD
P :
1. Inj AUGMENTIN 1.2gm /IV /BD
2. Tab AZITHROMYCIN 500mg PO/OD
3. Tab PAN 40mg PO /OD
4. Tab DOLO 500 mg PO / TID
5. Nebulization with IPRAVENT and BUDECORT every 6th hourly
6. Syp ASCORYL 10ml PO/ TID
7. Tab OLZIC 5mg / PO H/S
8. Tab PREGARALIN 75mg /PO / SOS
9. Vitals monitoring
10. Fever Charting 4th hourly.


Comments
Post a Comment